



Governor Jeff Landry Wants Louisiana to Lead with "Gold-Standard Science"
Meanwhile, the absence of "gold-standard science" behind LDH’s vaccine promotion reveals a serious breach of scientific responsibility.

We were thrilled on Friday when Governor Jeff Landry stated that 'Louisiana will prioritize gold-standard science to become the gold-standard state in the MAHA movement!' The statement on Friday was in response to comments made by HHS Secretary Robert Kennedy and National Institutes of Health (NIH) Director Dr. Jay Bhattacharya as seen in the video below.
When asked by a news host if we “Make America Healthy Again” by focusing on ingredients in foods and cereals, Bhattacharya responded:
“I think for something like this, a problem of this scope, it has to be an all of the above approach, certainly food, the drugs that we take, the lifestyle we live, and much else that science hasn’t really discovered yet. The way forward is to say what we know honestly, say what we don’t know honestly, and give excellent advice based on gold-standard science. As the Director of NIH, that’s exactly what I intend to focus the agency on: doing excellent science to improve the health of Americans.”
Gold-standard science refers to randomized, controlled clinical trials that are reproducible, conducted with ethical integrity, and carried out with full transparency.
We saw a glimpse of what a reliance on “gold-standard science” could look like last fall when Louisiana Surgeon General Dr. Ralph Abraham and Deputy Surgeon General Dr. Wyche Coleman took a stand against unethical and unscientific flu, COVID, and mask mandates in healthcare settings. They reinforced this approach when they announced that LDH would no longer promote flu, COVID, or mpox vaccination, but instead refer individuals to their family physician.
Research overwhelmingly indicates that flu, covid, and mpox vaccines are terribly flawed, carry significant risks, and are baselessly overpromoted as a general medical recommendation.
Because they are mandated annually for healthcare workers, the flu and covid vaccines are particularly grievous.
This recently released preprint from the Cleveland Clinic, Effectiveness of the Influenza Vaccine During the 2024-2025 Respiratory Viral Season, validates prior studies which indicate flu vaccination confers NEGATIVE efficacy, making the recipient more prone to illness.
“In an analysis adjusted for age, sex, clinical nursing job, and employment location, the risk of influenza was significantly higher for the vaccinated compared to the unvaccinated state (HR, 1.27; 95% C.I., 1.07 – 1.51; P = 0.007), yielding a calculated vaccine effectiveness of −26.9% (95% C.I., −55.0 to −6.6%).”
But what about the other vaccines, the ones routinely given to infants and children, as well as adults? The Louisiana Department of Health and the Surgeon General’s office stated they would continue to promote these vaccines and that was no joke. As measles cases in Texas and pertussis cases in Louisiana have been in the headlines recently, the support for these vaccines has been evident on social media posts and the LDH website.
In promoting measles and pertussis vaccination, the state is once again ignoring the lack of “gold-standard science.”
For example, as we have shared previously, no vaccine on the childhood schedule was licensed with an inert placebo-controlled clinical trial. The MMR-II vaccine had no placebo in the clinical trial - NONE - and was administered concomitantly (at the same time) with VARIVAX, a chicken pox vaccine. The other measles-containing vaccine, PRIORIX, was trialed with MMR-II as the “placebo.” The Informed Consent Action Network has reported that the MMR-II should have never been licensed. A FOIA they submitted returned information indicating that the FDA ignored the lack of a control group, the lack of sufficient number of study participants, and the significant number of adverse events.
“It [MMR-II] should not have been licensed because MMR-II was licensed by the FDA based on clinical trials which had a total of 834 children, had no placebo control, and only reviewed safety for 42 days after injection! Putting aside the lack of placebo control, even if the clinical trials were properly controlled, they did not have enough individuals to assess safety; nor did they review safety for long enough.
Despite the fact that approximately a third of the children in the clinical trials developed gastrointestinal issues and respiratory issues within 42 days of receiving MMR-II, due to their underpowered size and lack of follow-up, they were able to avoid this being a roadblock to licensure. Despite this vaccine being licensed, the clinical trials relied upon to license this vaccine clearly did not, as they could not, confirm that the product was safe, and certainly not for any period longer than 42 days, nor for even the 42 days they did review safety.”
This isn’t science, much less “gold-standard.”
Still, LDH states “the MMR is safe and effective,” a claim the manufacturer can’t even make. Additionally, LDH downplays the issue of vaccine adverse events while highlighting the complication of measles. Measles-containing vaccines are attenuated live-virus vaccines, meaning any complication associated with natural infection can also occur with the vaccine, as well as other serious complications.
Notice the measles vaccine side effects listed on the LDH website below: arm soreness, fever, rash, febrile seizures, severe allergic reactions.
In contrast, the following adverse events are listed in the MMR-II insert and include those identified during clinical trial or reported during post-approval:
Body as a Whole
Panniculitis; atypical measles; fever; headache; dizziness; malaise; irritability.
Cardiovascular System
Vasculitis.
Digestive System
Pancreatitis; diarrhea; vomiting; parotitis; nausea.
Hematologic and Lymphatic Systems
Thrombocytopenia; purpura; regional lymphadenopathy; leukocytosis.
Immune System
Anaphylaxis, anaphylactoid reactions, angioedema (including peripheral or facial edema) and bronchial spasm.
Musculoskeletal System
Arthritis; arthralgia; myalgia.
Nervous System
Encephalitis; encephalopathy; measles inclusion body encephalitis (MIBE) subacute sclerosing panencephalitis (SSPE); Guillain-Barré Syndrome (GBS); acute disseminated encephalomyelitis (ADEM); transverse myelitis; febrile convulsions; afebrile convulsions or seizures; ataxia; polyneuritis; polyneuropathy; ocular palsies; paresthesia; syncope.
Respiratory System
Pneumonia; pneumonitis; sore throat; cough; rhinitis.
Skin
Stevens-Johnson syndrome; acute hemorrhagic edema of infancy; Henoch-Schönlein purpura; erythema multiforme; urticaria; rash; measles-like rash; pruritus; injection site reactions (pain, erythema, swelling and vesiculation).
Special Senses — Ear
Nerve deafness; otitis media.
Special Senses — Eye
Retinitis; optic neuritis; papillitis; conjunctivitis.
Urogenital System
Epididymitis; orchitis.
Why does the manufacturer have to disclose this list of adverse events but LDH does not?
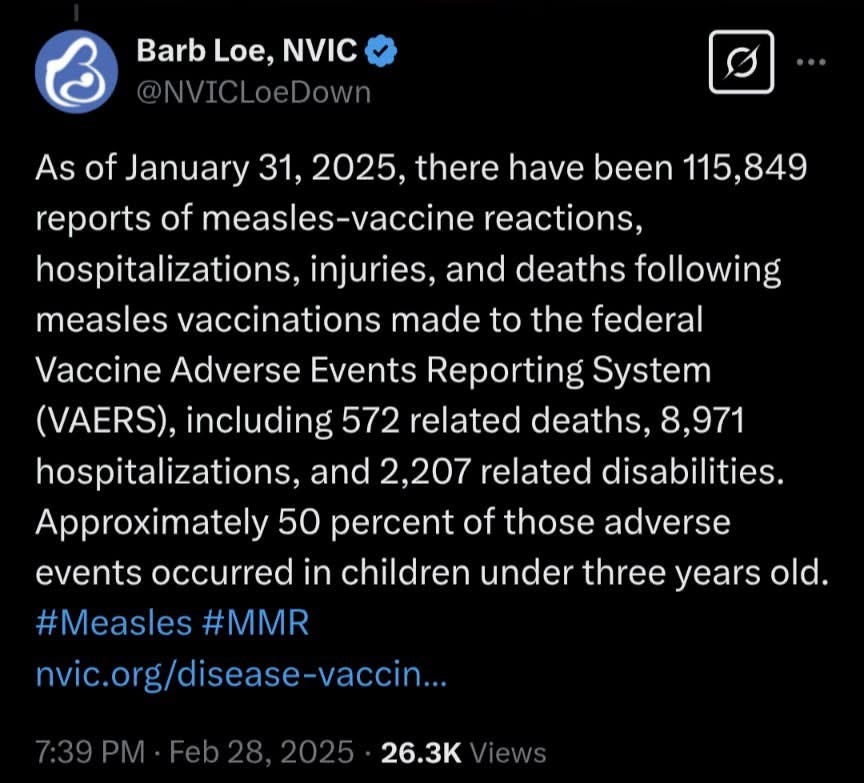
In contrast, MMR-associated adverse events reported to VAERS, the vaccine adverse event reporting system, indicate significant harm associated with MMR vaccination. Barbara Loe Fisher, founder of the National Vaccine Information Center, shared on Febraury 28, 2025, that 115,849 MMR-related reports to VAERS include 572 deaths, 8,971 hospitalizations, and 2,207 related disabilities.
What about whooping cough?
LDH has whooping cough, or pertussis, highlighted on the Immunization home page, as well, with extremely biased messaging. There are two DTaP — diphtheria, tetanus, pertussis — vaccines on the market for infants and children, Daptacel and Infanrix. Both were licensed using another vaccine, DTP, as the “placebo.” The DTP vaccine was the catalyst for the passage of the 1986 Act, the National Childhood Vaccine Injury Act (NCVIA). As vaccine manufacturers were being driven out of the market over lawsuits for vaccine-related injuries and deaths, they lobbied Congress for liability protections, thus the passage of NCVIA.
The DTP vaccine was taken off the U.S. market in 1996, but is still used in other countries. In a retrospective study conducted in Guinea-Bissau, data indicates a 10x increase in all cause mortality in girls and a 5x increase in all cause mortality in boys following DTP vaccine.

As dangerous as it is, the DTP vaccine was the “placebo” in the clinical trials for the two vaccines that took its place in the U.S. market and on the CDC recommended schedule.
This doesn’t pass for science, gold-standard or otherwise.
LDH again makes a claim that none of the pertussis-containing vaccine manufacturers do: “the whooping cough vaccine is safe and effective.” How is the safety of a drug determined that has never been tested against an inert placebo? And, no, the DTP vaccine clinical trial did not contain a control group, not even a fake one, when it was licensed.
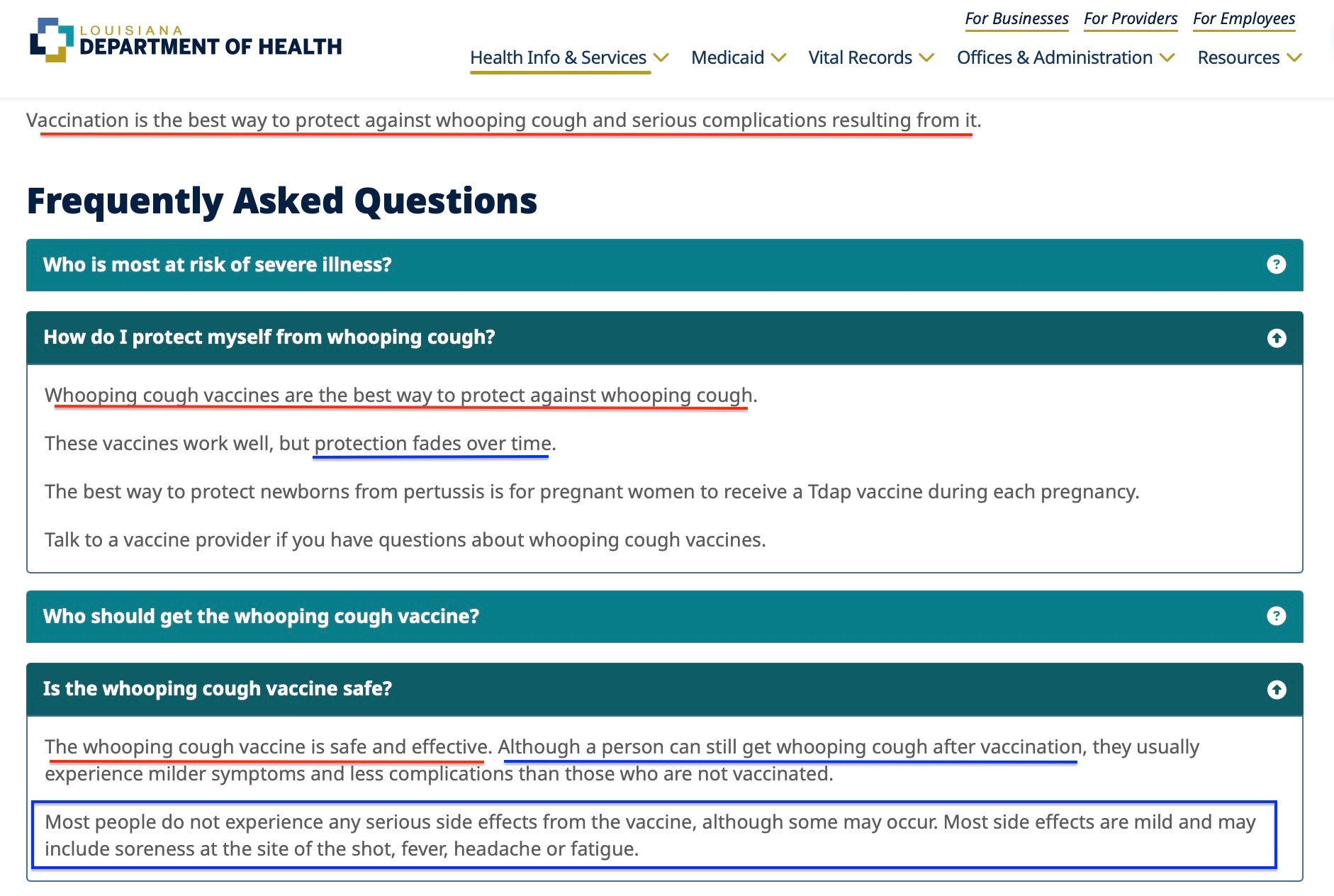
Several times on the website, LDH states that vaccination is the best way “to protect against whooping cough,” but also notes that “protection fades over time,” and “a person can still get whooping cough after vaccination.” As we noted in a social media post recently, studies indicate that pertussis vaccines do not prevent transmission or infection, but they also indicate that pertussis vaccination may make the vaccine recipient more susceptible to pertussis throughout their lifetime.

To support our claim we provided three studies that can be found in a document, Herd Immunity and Vaccination, on our website.
No pertussis-containing vaccine prevents infection or transmission of the bacteria.
“The observation that aP [acellular pertussis], which induces an immune response mismatched to that induced by natural infection, fails to prevent colonization or transmission provides a plausible explanation for the resurgence of pertussis and suggests that optimal control of pertussis will require the development of improved vaccines.” ncbi.nlm.nih.gov/pubmed/24277828
Being vaccinated with DTaP makes you more susceptible to pertussis throughout your lifetime.
“Because of linked-epitope suppression, all children who were primed by DTaP vaccines will be more susceptible to pertussis throughout their lifetimes, and there is no easy way to decrease this increased lifetime susceptibility.” https://pubmed.ncbi.nlm.nih.gov/30793754/
Infants are catching whooping cough from fully vaccinated siblings and adults.
“Conclusions: The incidence of pertussis was highest in children aged 12 years and under in this epidemic. At its peak, siblings were the most important sources of pertussis in infants 6 months and younger, particularly fully vaccinated children aged 2 and 3 years. Waning immunity before the booster at 4 years may leave this age group susceptible to infection. Even if cocooning programs could achieve full vaccination coverage of parents and ensure all siblings were fully vaccinated according to national schedules, waning immunity in siblings could provide a means for ongoing transmission to infants.” https://pubmed.ncbi.nlm.nih.gov/25391405/
Hospitals are requiring this shot for healthcare workers and students in the clinical setting even though it does not stop transmission or infection. Why?
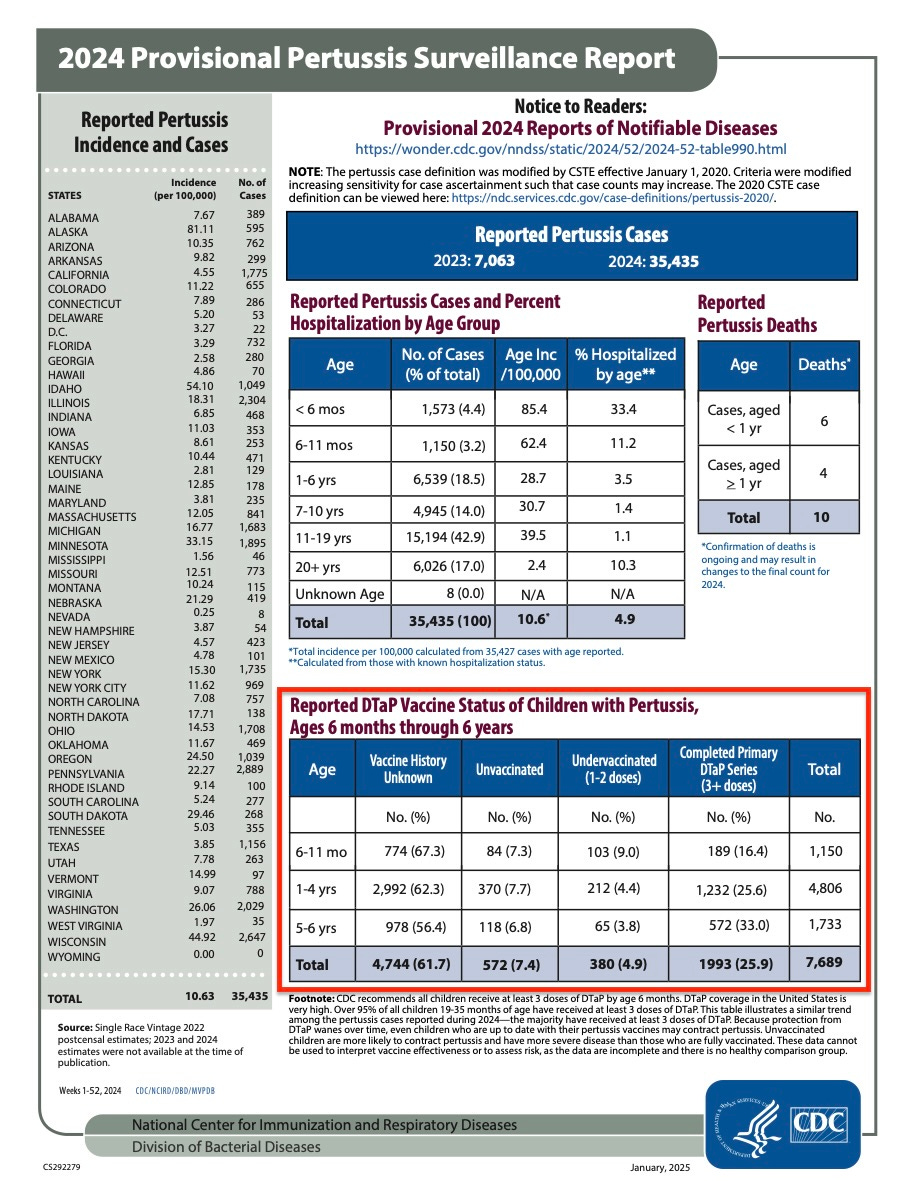
The CDC’s pertussis surveillance reports for the last several years indicate significant vaccine failure is going unaddresses while the drug is being mandated on healthcare workers.
Pertussis-containing vaccines are not without risks either.
Although LDH mentions minor side effects like sore arm, fever, headache, and fatigue, the inserts paint a different picture. The insert for Daptacel states: “A review by the Institute of Medicine found evidence for a causal relation between tetanus toxoid and both brachial neuritis and Guillain-Barré syndrome.” There is no pertussis-only vaccine — every pertussis vaccine option is in combination with tetanus.
The Daptacel insert also states: “Within 30 days following any dose of DAPTACEL, 57 (3.9%) [of 1,454] subjects reported at least one serious adverse event. During this period, the most frequently reported serious adverse event was bronchiolitis, reported in 28 (1.9%) subjects. Other serious adverse events that occurred within 30 days following DAPTACEL include three cases of pneumonia, two cases of meningitis and one case each of sepsis, pertussis (post-dose 1), irritability and unresponsiveness.”
In addition to the “study” results, post market surveillance reports include:
Blood and lymphatic disorders
Lymphadenopathy
Cardiac disorders
Cyanosis
Gastro-intestinal disorders
Nausea, diarrhea
General disorders and administration site conditions
Local reactions: injection site pain, injection site rash, injection site nodule, injection site mass, extensive swelling of injected limb (including swelling that involves adjacent joints).
Infections and infestations
Injection site cellulitis, cellulitis, injection site abscess
Immune system disorders
Hypersensitivity, allergic reaction, anaphylactic reaction (edema, face edema, swelling face, pruritus, rash generalized) and other types of rash (erythematous, macular, maculo-papular)
Nervous system disorders
Convulsions: febrile convulsion, grand mal convulsion, partial seizures
HHE, hypotonia, somnolence, syncope
Psychiatric disorders
Screaming
Would these vaccines have been licensed if “gold-standard” practices and standards had been required? No.
Have our children suffered as a result? Undoubtedly.
At last, the chronic disease epidemic in America is being acknowledged on a national level. It would be a serious oversight to ignore the crisis of medical and scientific ethics that created it. For decades, these drugs have been recommended, then mandated, for our children without meeting even the lowest standard of scientific research: a control group. We have only highlighted two vaccines today — MMR and pertussis-containing vaccines — but all vaccines on the CDC’s childhood schedule have the same serious scientific and ethical issues. None meet even the basic of scientific standards.
There is a reason we are striving for “gold-standard science” today - because it has been absent from our federal and state health agencies for decades. Acknowledging the harm that has resulted by accepting anything less is absolutely essential.
Don’t leave your family and friends without the information needed to fight for their health freedom! Click the button below and share Braving Freedom! 🇺🇸
Don’t forget you can listen to our articles on the Substack app!

Our advocacy is only possible with your help! THANK YOU!!